Nutrition Sciences Major Discusses Chronic Illness
Beatrice Glaviano ’26 discusses how she manages her ulcerative colitis and offers support to others who may also be facing health challenges, finding her true calling.
November 21, 2023
By Beatrice Glaviano ’26
Beatrice Glaviano’s experience with ulcerative colitis inspired her to want to help others.
This article contains graphic descriptions of illness, existential thoughts, and other hard topics. If this does not float your boat or you are not in the headspace to consume this content, please click out of this page. I prefer my readers to stay mentally well than to read my work. Thank you.
Welcome everyone to our first edition of the Chronically Ill Chronicles: a series dedicated to the life of a student trying to navigate college and life with chronic illness.
To start off, what the heck is chronic illness anyway? Is it like getting a supercharged version of the flu once a year? Superpowers with a drawback? Well...not exactly. According to Healthline, it’s defined as a long-term illness that usually cannot be cured (Chronically Ill: Definition, Patient Experience, Resources, and M, 2018), even though many can receive treatment over the course of their lives. Additionally, some chronic illnesses may predispose one to other illnesses, such as rheumatoid arthritis or other inflammatory diseases. Basically, it’s a sticky situation all around, and not the optimal place to be health-wise as a human being.
While I wasn’t asked specifically to write about my experience with ulcerative colitis (of which I’ll go into further detail about later), it is one of the main reasons why I fell in love with medicine in the first place. Without it, I doubt my life would be the same. So, let’s go back: early Fall 2013.
Figure 1: Beatrice (8 y/o). What an absolute nerd.
If you think I’m a nerd now, eight-year-old Beatrice was a whole different shade of Green Lantern. Magic Treehouse? Oh yeah. Legos? In surplus. The Amazing Spider-Man? Check. My entire room is a blindingly bright fuchsia, and my mom still has me going to dance lessons every Tuesday night at 6:15 p.m. Life was pretty good (though I was pretty sure my third-grade teacher had it out for me).
Little did I know that something else did.
It started with stomach aches, some nausea: classical signs of a stomach bug. According to the local pediatrician, I was going to be fine as the illness just needed some time to leave my body. It was just a stomach bug, after all – it would clear up soon enough.
Months passed.
The nausea soured, and hours were spent running back and forth from the bathroom to vomit. That was the first ER visit. “Tell us if it gets worse,” the nurse said. Diarrhea piled up in the toilet, stringy and mucus-filled. Blood leaked into it, too, uncurling as slow waves in the still water. Second visit. “If it gets worse, contact the doctor on-call.” One day, my mom asked me the last time I had peed. I didn’t remember. Could I pee? Did I forget how to pee? Oh my god. For the first time in my life, I flipped out. Eight years old, unable to urinate, and a destroyer of toilets: dear God.
Brief serious note: realizing that you may not remember how to pee is, rather frankly, terrifying. Please remind yourself to be grateful for your body, even if your relationship with it is rocky. Trust me on that.
And so, it continued: more diarrhea, more blood, more unanswered questions. After a while, I started losing count of how many times I watched the streetlights go by the car as we rode to the hospital again. Nothing. Weeks passed; I stayed curled up by the toilet vomiting for hours on end, praying to anything and everything that my tears on the fake tile floor were enough to convince the universe to have mercy on me. (I still have those moments, sometimes).
All I knew was the smell of my bowels and the acrid taste of vomit in my mouth. Was there a point where I wouldn’t? Was there a chance? At eight years old, I debated if being alive- in this state – was worth it. I didn’t really mean it of course, but given the circumstances...well, you couldn’t exactly blame me.
In total, the diagnosis took six months. Here are some things I remember:
I’m sitting in the doctor’s office, kicking my legs back and forth on the examination table. The memory as a whole is blurry; a nurse eventually walks in as my mother and the doctor wrap up their conversation. I’m put in a hospital bed and wheeled to an elevator. Apparently, I would be staying overnight for a while.
I remember falling asleep watching Episode III of Star Wars: Revenge of the Sith with my mom after getting an IV placed in. Fluids would help.
I remember a doctor telling me I could have my colon removed, and that I’d have a bag instead of an organ for the rest of my life. Being honest, my first thought was how I could never possibly wear a bikini – if I ever built the courage to, that is – with that bag.
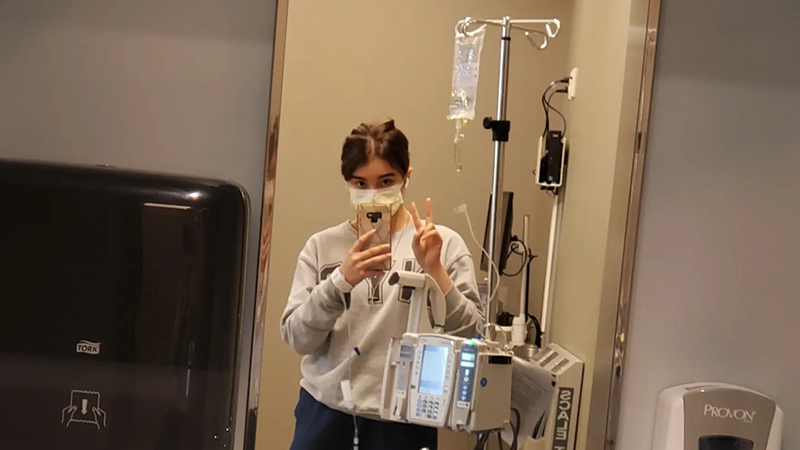
Beatrice Glaviano’s IV.
If there is one thing I do recall quite vividly, it was how much I smiled when I received my medication. Remicade, it was called; I’d be receiving a dosage of it every week until the disease was pushed into remission.
And eventually, it was. Granted, I couldn’t eat gluten or dairy for the time being, and I lost my popcorn movie nights, but it was better than dealing with any of the other stuff. Finding bread and pasta substitutes was pretty annoying, though.
Alright, now that you know my chronic illness villain backstory, what actually is ulcerative colitis (UC)? Well, it’s a form of IBD, AKA: inner bowel disease. This disease causes ulcers to grow along the intestinal lining of the colon – the large intestine – of the body and is usually passed down genetically. In my case, it was a recessive gene instead of the normal dominant. Hooray. Moving on, these ulcers are responsible for causing irritation to the intestinal wall, and they can also begin to bleed if irritated by passing substances like food.
[......]
Author: *clears her throat* “I don’t really know what else would be moving through the digestive tract of an eight-year-old. Maybe a tapeworm? God knows. Anyways – ”
Most of the general signs and symptoms of UC are what follows:
Diarrhea (with either mucus, pus, or blood, which are both signs of inflammation)
Abdominal pain
Fatigue
The need to use a bathroom in .01 seconds, and subsequently blowing up a toilet
Weight loss
The disease makes it so that your body is unable to properly absorb nutrients as basically anything you eat just runs through you
From my personal experience, a lack of appetite also comes about – though it’s not because of the nausea. It comes from the fear of getting nauseous; at points, it was better to not eat anything and feel less bad than to try eating something and chance blowing up the toilet. That’s just the truth. Even now, I still deal with some of this. Some nights, it’s like I’m eight again: balled up next to the toilet and trying to talk my body into some sense.
Ulcerative Colitis, looking over its Uno cards: “Vomit or draw 25” Me: ...Bro.
95% of the time, I lose. Sometimes it’s only an hour, sometimes it’s the entire night. Right now, it’s cleared up for the most part, but recently the boat did get a little rocked. You see, one of the big things they tell you with chronic illness is to not to get too stressed out, as that can aggravate it.
My doctor: “I know it sounds easier than done, but try making sure your stress levels stay as low as possible.”
Author, Pre-Med, Honors Program & Honor Society, working two jobs and slowly losing it: *Giggles* “I like your funny words, magic man.”
While I’m pretty good at managing my stress levels, over the past week they went through the roof. While I genuinely do love my classes and instructors, sometimes it can get a little much. It got so bad, in fact, there was blood in the toilet again after years of being in remission. Sometimes there would be spotting, yes, but nothing at this level.
Needless to say: I freaked out. My mind started to run a mental marathon: Would I need another colonoscopy? How much work would I miss? Would I miss a lab? Oh no, no no no. I ended up missing my A&P lab practical on muscles, and my lecture exam on Nervous Tissue. On that note, I am quite grateful that both of my professors are very understanding people, and that I was able to make these exams up. My instructors this semester are some of the best I’ve ever had in my life, and I couldn’t thank them enough for their teachings. Really. (If you all are reading this, I do mean what I say; you’re all fantastic).
Something that I’ve always battled with regarding my UC was the ‘what ifs.’ What if I didn’t have medical insurance? How fast would I deteriorate without meds? Remicade, for those who don’t know, is about 26k on the market. That’s like, tuition money people. Keeping me healthy, and while I do deserve the chance to live a quality life, I can’t help but occasionally think that I need to make my “money’s worth” during my time here on Earth. (Does that sound bad? That might sound bad. I promise I’m in therapy).
Anyways, there are other factors that live in my head in regard to the disease, and they’re not only fantastic. However, it was because of UC that I gained a love for medicine, for patient care, for empathy and patience with those who are suffering because I understand that. Oddly enough, being able to relate to patients who are going through similar things or are scared that they haven’t received a diagnosis is one of the best things the disease has given me (aside from accommodations for a single dorm/apartment on-campus).
For the sake of HIPAA, I will keep this person’s name anonymous, but let me tell you something that happened in the ER over the summer. Let’s call the patient Sally. Yeah, that’ll work.
It started with a loud expletive (as most interesting things do). It was this woman, surely in her late 60s or early 70s, being worked on by some of the techs for whatever reason.
“Oh my god, I’m sorry. I didn’t mean to say that aloud,” she explained (this was followed by more cussing, of course, to our amusement).
If there’s anything that puts some fun into the ER, it’s interesting patients who have common decency and the mouth of a sailor. Immediately, I liked her. Part of my job description as a volunteer was to talk to patients, and while I’m a little scared of geriatrics, I decided to walk on over.
“Hi, I’m Beatrice.”
“Sally.”
We shook hands, and I took a seat next to her.
“So, what’s going on?” I asked.
Apparently, she had been going through some abdominal pain and had absolutely no clue what was happening. It was very painful for her, clearly, but she was managing it well overall. As a group, geriatric patients tend to have less of a pain response so much so that when they do feel pain, eyebrows should be raised. More than this, though, was that she had a M.S. in Criminology (or something similar; the memory is hazy). She has two kids, and has lived in New Haven for most of her life. Sally is also a fan of documentaries, specifically National Geographic and David Attenborough.
I love patient backgrounds. It’s what gives them life, character, meaning; it’s what makes the role of a doctor so magical: you’re being trusted with not only the anatomy and physiology of someone, but their soul too. And in that moment, I was that person. Frankly, I was initially really nervous. Was the age gap too much? Would my humor come off wrong? Would I be irked by something?
No. Not at all, not in the slightest.
We chatted for an hour, giggling over the biohazard signs and mentioning how lovely they were at this time of year. There were serious moments, though.
“Why is it taking so long?” She asked, facing to look over at me with big, life-filled eyes. “Aren’t doctors supposed to know what to do?”
And, immediately, I was eight again, staring back at her.
“Well...” I started. I had to handle this delicately, and professionally. How to do that? No clue, but no better time than now. “Truthfully, the doctors don’t always know what’s going on.”
Sally looked at me, suddenly looking older than she was a minute ago. Wow, that was encouraging. Great job, Beatrice.
“Physicians spend their lives learning about the human body – the anatomy, the physiology, medications, treatments, cures, diseases.” I explained to her slowly. “Your doctors don’t want you to be in the ER. They want you to get better as soon as possible; but they can’t do that unless they know exactly what’s going on.”
Her eyes softened a little bit, and I continued.
“If your physicians make a judgment call too quickly and misdiagnose you, they may make things worse. They are taking their time to ensure that they help you instead of harming you.”
Sally looked at me in what seemed like shock, and I felt called to tell my story. Was I supposed to? Probably not, but I’d also told a patient to their face that doctors don’t always know what’s going on (because who actually does?) while they were in the ER. I digress.
“I just...I get it, dude.” I told her (yes, I called a 60-year-old patient ‘dude’) after I explained my situation. “I get frustrated at the lack of answers, being scared. I understand it. I also understand that this ER is freezing cold.” We laughed at that. “And that it’s less than optimal, despite the biohazard signs.”
“Well, what I’m going through is nothing in comparison,” she replied.
I raised an eyebrow. “Who said that? People say to never think that you’re ‘better’ than someone, but that also applies to being ‘worse.’ What’s the point of that? You are here because you are going through something, and we are here to help you get better.”
And that’s when I realized something.
In pre-med, they tell you that book medicine is different from that of real life. The books tell you what to do, yes, but they don’t prepare you for everything. What do you do when a child is screaming because of an infection, and you can only tell the mother to wait for test results? How do you handle a geriatric patient who is ready to pass on, but their family is not ready to let them go? How, should the worst happen, do you remember that it’s not your fault? In what way do you convince yourself to take a hot shower while trying to wipe a memory that only smears?
How do you remember that?
You see, medicine isn’t just bare examination room walls and a crisp set of surgical tools: it’s about life as it is as much about death. There will be loss and sacrifice, but there will also be victory. Your patient gets to remission, their scans are clean, and you can see the stress lift off of the family’s shoulders. You get a really dope paycheck (because c’mon, that’s also a benefit) and decide to spend it on a collector’s Lego set. You are smiling and crying as you read that acceptance letter because let me tell you:
Realizing that you are meant to do something for the rest of your life is a big moment. I’m 19, dude, and as much as I complain about my joint pain and alarming coffee habits, I’m pretty young in the grand scheme of things. The trees that grow next to my dorm will probably outlive me, as well as some random tortoise in the Galapagos Islands.
When I was with that patient, for once in my life there was no question about what I was doing. The thoughts that had been buzzing in the back of my head, ones of ‘you’re going to be horrible at patient contact’ or ‘you won’t be able to handle it’ were silenced.
If I could use my life experiences as someone with an incurable illness to help someone understand what’s happening, then perhaps everything was worth it after all. I know that this article has been rather a doozy to read through, and if you’ve made it to the end, I’m glad you stuck around. I’ve been writing this bad boy for a few days now, and I didn’t expect it to get so long. I hope that this piece helps anyone who’s struggling with their own medical situations, or who are looking for a sign of inspiration toward medicine.
If you want to do it, go pre-med. I promise you won’t regret it (also, the University has a great pre-med program).
I hope everyone is having a fantastic week and staying as healthy as possible (people are getting sick left and right, as it ‘tis the season). Please feel free to reach out to me at BGlav1@unh.newhaven.edu or my personal email, beatriceg2022@gmail.com regarding questions, blog ideas, or commentary. Take care everyone, and stay warm.
Peace, love, and all the PB,
Yours truly,
Beatrice